Most B2B campaigns targeting hospitals start with the wrong question.
The wrong question is: “Which hospital should I target?”
The right question is: “Which person inside that hospital has the authority, the budget, and the reason to act on my offer right now?”
These are completely different questions. And the answer to the second one changes everything about how you build your contact list, what you say in your email, and who you follow up with.
A typical hospital purchase in 2025 involves around 9 decision-makers and influencers before a deal closes. The average healthcare technology buying cycle runs about 12 months. And by the time a hospital contact officially reaches out to a vendor, they are already roughly 70% through their decision-making process. That means most of the evaluation, comparison, and internal discussion happens before you even know a deal exists.
The vendors who win hospital accounts are not the ones with the best product pitch. They are the ones who reached the right people at the right level, with the right message, before the formal process locked the field.
This guide breaks down exactly how to do that for the three most commercially important hospital contacts: the Chief Medical Officer, the procurement director, and the hospital administrator.
What is a hospital email list by role?
A hospital email list by role is a segmented B2B contact database where contacts are filtered by specific job function within the hospital, not just by the institution they work for. Instead of a broad list of hospital contacts, you receive targeted lists of CMOs, procurement directors, procurement managers, or administrators specifically. Role-based segmentation lets you match your message to the person whose priorities align with what you are selling, which directly improves response rates and lead quality.
The Hospital Buying Committee: Who Does What

Before targeting any role, you need to understand how they fit into the buying process. Hospital purchasing decisions rarely start at the top and flow down. They usually start in the middle and flow in all directions at once.
Here is how it typically works for a mid-to-large hospital:
A department head, a clinician, or an administrator identifies a need. That request moves to the procurement team for vendor evaluation. Procurement shortlists suppliers and brings in the relevant clinical or operational leader, such as the CMO or CNO, to validate the fit. The CFO reviews the financial case. The CEO approves the final commitment.
Knowing where your product fits in that chain tells you which role to start with and which roles need to be in your campaign simultaneously.
Role 1: The Chief Medical Officer (CMO)
Who is a Chief Medical Officer in a hospital?
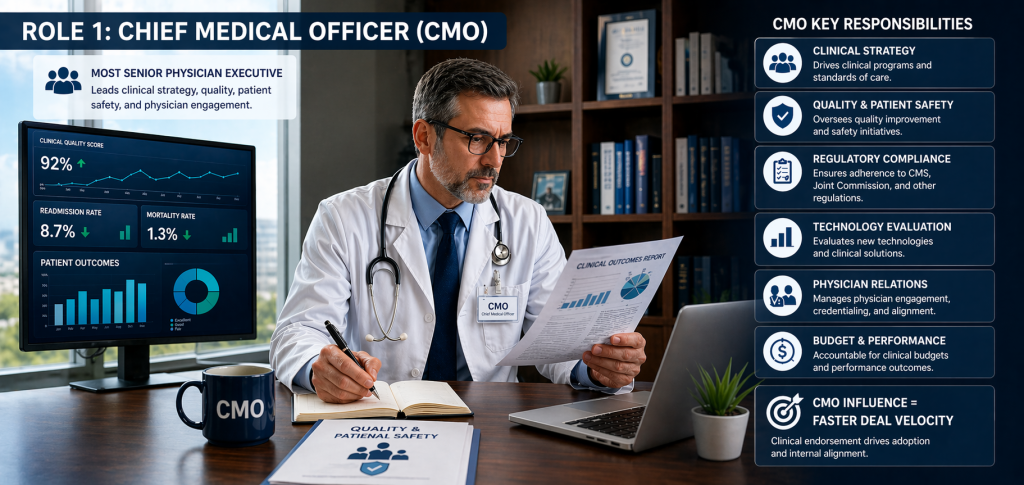
The Chief Medical Officer is the most senior physician executive in a hospital. They are responsible for clinical operations, quality programs, patient safety, physician relations, clinical strategy, and regulatory compliance. According to research published in PubMed, the CMO “plays a major role in advising the administration regarding clinical equipment purchases, including those for emerging technologies.” There are over 14,500 CMOs across the United States in 2026.
What does a hospital CMO do day to day?
The CMO sits at the intersection of medicine and management. On any given day they are overseeing quality improvement initiatives, managing credentialing and physician relations, ensuring compliance with CMS and Joint Commission standards, and evaluating new clinical technologies for adoption. Many CMOs now also hold direct budget accountability for clinical departments, which means they are in staffing and finance meetings as regularly as clinical committee meetings.
An important detail many B2B marketers miss: the CMO is not purely a clinical figure. They are evaluated on operational and financial outcomes just as much as clinical ones. Reducing readmission rates, controlling pharmacy costs, improving patient safety scores, and managing the efficiency of clinical workflows all fall within their scope.
How does a hospital CMO influence purchasing decisions?
CMOs rarely make final purchasing decisions alone. What they do is validate the clinical case for a product, guide the pilot program design, chair or influence technology assessment and formulary committees, and provide the clinical endorsement that moves a product from evaluation into formal procurement.
Think of it this way: a medical device or clinical software product that the CMO endorses has a clear internal champion. One the CMO is neutral or skeptical about faces a much longer and harder path through procurement and finance. Their influence is a multiplier on your deal velocity.
What products and services should target the CMO?
Medical devices, clinical software, EHR solutions, patient safety tools, digital health platforms, AI-assisted decision support systems, diagnostics, and any product where clinical outcomes and workflow integration are the primary evaluation criteria. If your product touches patient care in any way, the CMO is a relevant target.
How do you message a CMO effectively?
This is where most vendors get it wrong. They lead with features or operational benefits when talking to a physician executive who evaluates products through a clinical lens first.
What works with CMOs:
Lead with clinical evidence. A CMO who endorses a product in committee needs to defend that endorsement to the medical staff. Give them the evidence they need to do that: peer-reviewed data, outcomes from comparable institutions, clinical validation results.
Frame the business case second. Once the clinical case is established, add the operational and financial angle: reduced length of stay, fewer adverse events, lower readmission penalties. CMOs respond to data that shows their clinical values and the hospital’s financial health moving in the same direction.
Be specific to their institution type. A CMO at an academic medical center cares about different metrics than a CMO at a community hospital. Academic centers focus on research integration and teaching. Community hospitals focus on accessible, efficient care. Referencing their specific context in your outreach signals that you understand their world.
Keep the email short. CMOs are high-volume inboxes with limited time. A 400-word email will not be read. A focused, four-sentence email that identifies a specific clinical challenge and offers a clear next step will be.
Connect with verified hospital CMO contacts here.
Role 2: Hospital Procurement Directors and Procurement Managers

Who is a hospital procurement director?
The procurement director manages the vendor evaluation and approval process for the hospital. They control which suppliers enter the formal buying process, oversee RFP issuance and response evaluation, negotiate and manage vendor contracts, and ensure the hospital’s purchasing activities comply with its own policies and applicable regulations.
In a large health system, the procurement team is often structured with a director setting policy and strategy, and procurement managers handling day-to-day purchasing, contract administration, and vendor communications.
What does a hospital procurement director do?
Supply chain costs represent 25 to 30% of total hospital operating budgets. The procurement director is responsible for managing those costs while maintaining supply continuity, vendor compliance, and contract performance. In 2024, 62% of US hospitals implemented data-driven procurement systems, which means procurement directors are increasingly technology-informed buyers who respond to data-driven vendor pitches.
Their core responsibilities include managing GPO (Group Purchasing Organization) relationships, running RFP processes for major supplier categories, evaluating vendor financial stability and compliance documentation, and managing the hospital’s approved vendor list.
Do hospital procurement directors approve vendor contracts?
Yes, within defined thresholds. Most hospitals have a tiered approval structure where procurement directors approve contracts up to a certain value, with the CFO or CEO required for larger commitments. For most B2B vendors selling products in the mid-market price range, the procurement director and their team are the primary approvers.
When do hospitals require RFPs vs. sole-source procurement?
Hospitals require competitive RFPs for purchases above a defined spending threshold or for contract categories involving multiple qualified vendors. The average hospital RFP takes between 9 months and 3 years to complete depending on contract complexity, budget cycle timing, and regulatory requirements.
Sole-source procurement is used when only one vendor can reasonably meet the specification, typically requiring formal justification and sign-off above the procurement director level. For most vendors, the RFP is the path they will need to navigate.
This timeline has a significant strategic implication: if you are not in front of procurement before the RFP process starts, you are already behind. Vendors who reach procurement directors with relevant, credible outreach before the formal evaluation period begins have a meaningful advantage over those who first appear in the RFP response queue.
How do you message a procurement director effectively?
Procurement directors respond to an entirely different pitch than CMOs. Clinical outcomes are not their primary lens. They evaluate vendors on commercial terms, process efficiency, risk management, and total cost of ownership.
What works with procurement directors:
Lead with the commercial case. Cost reduction, pricing transparency, contract flexibility, and favorable terms relative to comparable vendors. If your product integrates with the hospital’s existing systems or GPO contracts, say so immediately.
Demonstrate compliance readiness. Procurement teams care about a vendor’s ability to meet regulatory and documentation requirements. Mentioning your compliance certifications, your experience with hospital RFP processes, and your reference accounts at comparable institutions signals that you understand how procurement works.
Address the risk conversation early. Procurement directors manage vendor risk. Any new supplier relationship carries onboarding risk, supply continuity risk, and financial risk. A vendor who proactively addresses these concerns in the initial outreach stands apart from one who only talks about product benefits.
Make the next step easy. Procurement directors receive a high volume of vendor outreach. An email that asks for a 30-minute call with no context generates friction. An email that offers a one-page product summary, a reference account list, and a brief conversation about whether there is a fit removes it.
Access the hospital procurement email list here.
Reach procurement managers specifically here.
Role 3: Hospital Administrators

Who counts as a hospital administrator in B2B marketing?
Hospital administrators cover a broad range of operational leaders: chief administrative officers, hospital directors, department managers, facility managers, and operations executives responsible for the day-to-day running of the hospital. In smaller hospitals, the administrator may function as the primary decision-maker across multiple purchasing categories. In larger systems, administrators manage specific functions like IT, facilities, human resources, or patient services.
What does a hospital administrator do?
Administrators oversee budgeting, establish and enforce procurement policies, manage departmental operations, and hold purchasing authority within their defined area of responsibility. Research consistently shows that hospital administrators wield significant influence over purchasing decisions even when they are not the final contract signatory. They also initiate many vendor searches by identifying an operational gap or need and beginning the internal discussion that eventually becomes a procurement evaluation.
Do hospital administrators approve vendor contracts and budgets?
Within defined thresholds, yes. The hospital medical director’s explanation of how hospital buying works is useful here: unit managers and department administrators approve minor equipment purchases and supply vendors. Administrative directors handle more significant purchases. The CEO and CFO approve major capital commitments. For most B2B vendors, the administrator tier is where the initial vendor relationship begins and where operational fit gets established.
How do you segment hospital administrators by type?
Not all administrators are the same audience. Your segmentation approach should reflect the operational context of the hospital type:
Academic medical centers are large, research-oriented institutions with complex administrative structures. Multiple administrators manage different functional areas. Relevant for technology, research infrastructure, and services that support both clinical and educational operations.
Community hospitals serve regional populations with leaner administrative teams. Decision-making is more centralized. The administrator often has broader authority across multiple categories.
Rural and critical access hospitals operate on tighter budgets with smaller teams. Cost efficiency and operational simplicity are the primary evaluation criteria for any new vendor relationship.
Teaching hospitals blend clinical, educational, and research functions. Administrators here coordinate across multiple stakeholder groups and are particularly attuned to compliance and accreditation requirements.
Private health systems often have standardized procurement processes across facilities. Getting into a health system’s approved vendor list can open multiple facilities simultaneously.
How do you message hospital administrators effectively?
Administrators respond to operational language. They think in terms of efficiency, cost, compliance, and the ability to implement without disruption.
What works with administrators:
For facilities, operations, and services vendors: lead with cost reduction, process efficiency, and operational impact. Quantify the benefit wherever possible. “Reduces maintenance callouts by 30%” is more actionable than “improves facility management.”
For IT and SaaS vendors: lead with integration simplicity, security compliance, and staff adoption. Hospital IT environments are complex and administrators are risk-averse about anything that disrupts existing workflows. Demonstrating that your product fits into their current systems rather than replacing them reduces a major objection.
For process-improvement tools: frame the value around measurable outcomes the administrator is already being evaluated on. Billing cycle time, compliance audit results, staff efficiency metrics. Connect your product to the numbers they report upward.
For all administrator outreach: be concrete, be brief, and make the ask specific. Administrators manage a high volume of operational demands. An email that clearly states what you offer, what problem it solves, and what you are asking them to do next respects their time and is far more likely to generate a response than one that requires them to read through five paragraphs to understand what you are selling.
How to Map These Three Roles Into a Single Campaign
The most effective hospital B2B campaigns do not treat these roles as separate audiences. They treat them as a buying committee where each contact needs to be reached with a different message about the same product.
Here is a practical framework:
Start with procurement. The procurement team owns the formal evaluation process. Getting into a conversation with procurement before the RFP cycle opens is the single biggest competitive advantage available to a hospital vendor. Use the procurement email list to initiate an early-stage conversation about your product category before a formal need is publicly declared.
Move to the clinical or operational validator. Once procurement shows interest, the relevant validator enters the picture. For clinical products it is the CMO. For nursing technology it is the CNO. For IT it is the CIO. For facilities it is the administrative director. Use role-specific messaging that speaks directly to what this person cares about professionally.
Keep the administrator informed. Administrators often initiate vendor searches and track the progress of evaluations within their area. Keeping them aware of your conversations with procurement and the clinical validator prevents your deal from stalling because the person who started the process feels left out of it.
Escalate to the CEO or CFO for high-value deals. For contracts above the administrator or procurement director approval threshold, the CFO reviews the financial case and the CEO approves. A separate, brief executive-level communication that frames the business impact of the investment, not the product features, is what reaches this tier.
The hospital CEO email list and the chief executive officers list cover this executive escalation layer for campaigns that require board-level awareness.
What Data Do You Need for Each Role?
The data fields that matter shift by role:
For CMOs: Full name, verified email, direct phone, hospital name and type, health system affiliation, specialty area, NPI number, years in role.
For procurement directors and managers: Full name, verified email, direct phone, job title (director vs. manager distinction matters for message targeting), hospital name, bed count, GPO affiliation, geographic targeting fields.
For administrators: Full name, verified email, direct phone, exact title, hospital type (academic, community, rural, private), department area, hospital revenue and employee count.
Hospital bed count is particularly useful for administrators and procurement. A 50-bed critical access hospital operates on a different budget, timeline, and approval process than a 700-bed regional medical center. Messages that do not account for this difference will consistently miss the mark at one end of the size spectrum.
Are Hospital Email Lists GDPR and HIPAA-Compliant?
HIPAA does not apply to B2B marketers emailing hospital executives. HIPAA governs protected health information about patients and applies to covered entities. A vendor emailing a CMO about a clinical software platform is not handling patient data and is not a covered entity. HIPAA becomes relevant only if your outreach involves patient records, which a professional contact list does not.
CAN-SPAM governs US-based outreach and requires honest sender identification, no misleading subject lines, a physical address in every email, and a working unsubscribe mechanism honored within 10 business days. GDPR applies to EU-based contacts and permits B2B outreach under the legitimate interests basis when the message is professionally relevant and includes a clear opt-out.
Hospital IT environments run aggressive spam filters. Large hospital systems often use catch-all domains, which means bounce notifications do not always signal an invalid address. This makes working with a verified list sourced from professional directories and validated through real-time SMTP checks significantly more important than it is in other B2B categories.
Frequently Asked Questions
Who is a Chief Medical Officer in a hospital? The CMO is the senior physician executive responsible for clinical operations, quality, patient safety, physician relations, and clinical strategy. They advise hospital administration on clinical equipment purchases and evaluate new technologies. There are over 14,500 CMOs in the US in 2026.
How does a hospital CMO influence purchasing decisions? CMOs validate clinical claims, guide pilot program design, and chair or influence technology assessment committees. Their endorsement accelerates product adoption across service lines. They do not typically sign contracts independently but are often the critical internal champion a vendor needs to advance through procurement.
What does a hospital procurement director do? They manage the vendor evaluation process, own RFP issuance and response evaluation, negotiate supplier contracts, and maintain the hospital’s approved vendor list. Supply chain costs are 25 to 30% of total hospital operating budgets, making procurement directors some of the most commercially significant contacts in hospital B2B marketing.
What does a hospital administrator do? Administrators oversee daily hospital operations, budgeting, and procurement policy within their functional area. They hold purchasing authority within defined thresholds and frequently initiate the vendor search process when they identify an operational gap.
How many touches are needed to get a reply from a hospital CMO or procurement director? Industry benchmarks for cold B2B outreach to senior healthcare executives typically point to 6 to 8 touches across multiple channels over 2 to 3 weeks before a meaningful response rate is achieved. One email rarely works on its own. A structured follow-up sequence, where each message adds a new angle rather than repeating the original pitch, consistently outperforms single-send campaigns.
How to avoid spam filters when emailing hospital administrators? Authenticate your sending domain with SPF, DKIM, and DMARC records before any campaign. Warm up new sending domains gradually. Keep your daily send volume under 100 emails per sending address. Use verified contact data rather than generic role-based inboxes like procurement@ or info@. Hospital IT teams run some of the most aggressive spam filtering of any industry.
What subject lines work best for hospital executive outreach? Specificity beats cleverness. A subject line that references the recipient’s hospital type, a current operational challenge, or a concrete outcome delivers better open rates than a generic headline. Keep subject lines under 50 characters for mobile readability. Avoid trigger words like “free,” “guaranteed,” and excessive capitalization that activate spam filters.
How to use ABM to target multiple decision-makers in one hospital system? Build separate contact lists for each role within the same target accounts. Develop role-specific messaging that speaks to each contact’s priorities independently. Coordinate timing so that different team members reach different contacts within a two to three week window. The goal is for multiple stakeholders inside the same institution to receive relevant, credible outreach from your organization at roughly the same time, which builds internal familiarity before any formal evaluation begins.
Start Reaching the Right People in the Right Roles
Hospital B2B marketing fails when it treats the hospital as a single audience. It succeeds when it reaches the right person, at the right level, with a message built for their specific role in the buying process.
Prospects Influential builds role-specific hospital contact lists from verified, sourced data with over 30 years of healthcare list brokering experience across the US and Canadian markets. Whether you need CMO contacts for clinical outreach, procurement professionals for vendor evaluation conversations, or administrators for operational product campaigns, the right list starts with choosing the right role.
The hospital procurement email list and procurement managers email list cover the vendor evaluation layer. The healthcare professionals list covers clinical and operational leaders including CMOs. The hospital CEO email list covers executive-level awareness and approval.
Get in touch with Prospects Influential to discuss which combination fits your campaign You can also read how precision targeting applies in other B2B contexts in our guides to manufacturing company outreach strategy and email best practices for niche industry campaigns.